
A long search for a cure for beriberi in Southeast Asia in the late nineteenth century was led by trial and a lot of error
Nia Deliana
Before the Dutch scientist and physician Christiaan Eijkman discovered the cause of beriberi in 1896 (for which he was awarded a Nobel Prize in 1929), the treatment of patients with this condition in colonial societies in Netherlands Indies, Malaya and Singapore had been left to trial and error, mostly leading to dead ends. After Pasteur and Koch revolutionised medicine with the germ theory of disease in 1870, attempts were made to find the germ responsible for the spread of beriberi. For many decades, these approaches would ultimately see ongoing suffering particularly among communities on the margins of society – coolies, soldiers, and prisoners in the colonies – even in the midst of significant medical endeavour.
One disease among many
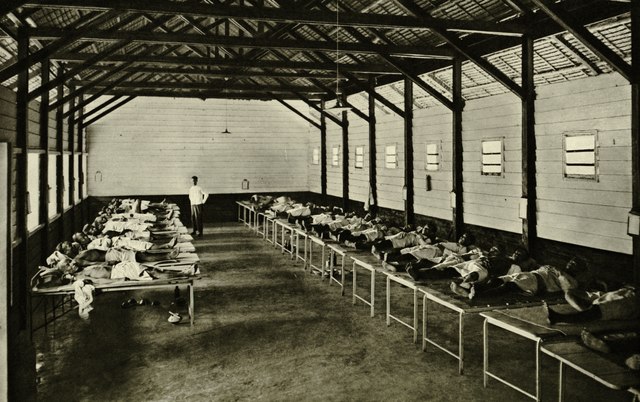
A severe outbreak of beriberi in Malaya was first observed in 1848. Two decades earlier, Bankier, a naval surgeon in India, had listed the symptoms of the disease to include paralysis of the muscular and nervous system, chest pain, spinal cord problems, chronic cough, kidney failure, water retention, fever, and bowel conditions. British colonial reports issued between 1886 and 1901 noted tens of thousands of deaths in Sumatra, Malaya and Singapore during that time. These included reports from Dr A. W. Sinclair, who served as the Selangor State surgeon from 1882-1888, and Dr Leonard Braddon serving in that state as District Surgeon. Both reported a particularly heavy toll amongst foreign workers, known as coolies, largely brought in to work on the colonies’ plantations, where they were supplied with food as cheaply as possible.
Unclear diagnosis was prevalent due to the range of symptoms in common with other endemic diseases, and its causes remained largely a mystery throughout the nineteenth century. In Malaya, the British middle class strongly believed that the origins of the disease stemmed from within the unhygienic and illiterate native populations, and so the medical measures taken were highly racialised. Medical inspections, treatments, and curfews were centered on the dwellings of the native populations only.
Lockdowns and quarantine processes were implemented and maritime borders were closed, gravely impacting the colony’s local economy. Ships loaded with thousands of coolies – largely from China and India – and soldiers and prisoners transported by the British to work in plantations areas, were denied entry. Enforcing such public health regulations was not easy. During this period, colonial authorities in Malaya and elsewhere in the region faced ongoing unrest from the indigenous populations. Loose immigration controls at the borders also meant there was a thriving smuggling route, and workers continued to head to coolie camp settlements and plantations. Beriberi and other diseases were prevalent throughout these settlements.

Between 1848 and the 1920s, beriberi spread largely unchecked across settlements and plantations in Singapore, Malaya, and the Dutch East Indies, triggered by the expansion of a plantation economy and a highly mobile workforce. This was not through want of trying to stop it. Similar patterns of medical interventions were adopted across the British and Dutch colonies in efforts to curb its spread, though mostly with little or only temporary effect.
Regulations and remedies
As early as 1850 The Singapore Free Press and Mercantile Adviser newspaper reported the implementation of quarantining at the maritime border and lockdowns in an effort to limit the spread of the disease in the city. 250 Indian British paid soldiers called sepoys and coolies from India and China were denied entry to the island and were instead forcibly relocated to remote work sites and settlements such as one in Tanjung Kubong, Labuan Island. The colonial government built a hospital with financial support from the coolies and soldiers themselves, and various doctors and scientists conducted examinations and experiments here in their search for remedies for the disease.
The sick sepoys living in military barracks on the Labuan Island testified that drainage and sanitary problems were the cause of several diseases within the settlement at the time, including beriberi. Their findings led to the introduction of changes to diet in the camp, including the addition of fresh vegetables and animal proteins, which had previously been in short supply. Other measures that were believed to have made a positive impact on the health of the residents included salt water intake, improved access to fresh air and ventilation in the hospital and dwellings, and clearing the jungle from around the settlements. This approach was in keeping with the popular new sanitation theory, of which Florence Nightingale was a well-known proponent at the time.
Whilst the disease was not altogether contained it did bring about a temporary improvement in conditions, which allowed the British to re-open the borders to incoming economic activities. The regions subsequently witnessed an influx of laborers, industry and production activity in the mining and plantation sectors. In less than a decade, the numbers of Chinese and Indian laborers in the colony had grown fivefold. In Perak for instance, the number of laborers from mainland China alone increased from 9,000 to 50,000 people between 1877 to 1883.
The illness soon returned. In August 1879, there was another severe outbreak of beriberi in Singapore. Although the medics called for numerous measures to contain the spread, the disease would not be halted unless the main sources of infections were targeted. Plantation camps where coolies, soldiers, and prisoners lived were once again quickly identified as centres for the spread of the disease, but coordination of public health interventions across the regions remained difficult and greatly hindered efforts.
In the same year, a similar outbreak struck communities across the Malacca straits in Aceh. The categories of patients recorded as suffering from the disease were the same as those in Singapore and Malaya, although the number of ill soldiers and prisoners was relatively higher. Patients were treated in Aceh’s capital, Koeta Raja. Throughout the 1880s, Aceh was ridden with tragic loss caused by war and a tsunami that struck the region in 1886. Plantations in Deli where coolies, convicts and soldiers camped in poor conditions were so terribly afflicted with beriberi that the petroleum industry and wider local economy in Langkat suffered huge losses.
Polished rice and salted fish
Both the British and Dutch colonial governments expanded the number of hospitals in their colonies and tasked scientists and doctors with the search for a remedy. Imported salted-dried fish, polished rice, adulterated ghee and tinned milk were identified as sources of the disease. These were foods commonly detected in the diets of coolies, soldiers, and prisoners, the groups most afflicted by the disease.
In 1879 when the Deli area experienced a significant beriberi outbreak, investigations identified trichina poison found in salted-dried fish as a key cause. Experiments in which scientists examined groups both with and without the disease, pointed to the consumption of the fish as decisive factor and again prompted a directive to change in diet. In 1879 the Singapore Daily Times reported that Dr Gelpke, a Dutch military officer who conducted medical research and experiments on beriberi patients in the area, had concluded that the main trigger was caused specifically by eating certain kinds of imported dried fish from Siam where the disease was endemic. In place of the imported salted fish he recommended the addition to diets of a dried meat called Deng deng (Dendeng), fresh fish and salted eggs.
In response to these findings some changes were made to conditions in the plantations and camps and the overall number of cases across the colonies declined. Nonetheless, throughout the 1880s the disease remained prevalent. On 12 March 1883 an article in The Strait Times reported that the British colonel, Frederic Brine and his delegation visited a military hospital close to Pante Pirak bridge in what is now Banda Aceh, which included a special ward for beriberi patients.
At around the same time, a major outbreak of beriberi among 9,000 coolies living in Teluk Anson in Perak, Malaya was blamed on the non-nitrogenous boiled rice they were supplied. Hospitals were erected to treat the sick workers with the cost then passed on to the families of the coolies themselves. Yeng Wah hospital in Perak, built and operated to take care of the Chinese coolies working the region, treated at least 3,000 patients each year between 1880 to 1883. The hospital was funded by a tax deducted from their salaries at a rate of three dollars a month.
During the 1880s across the colonies of Malaya, Singapore and Netherlands East Indies, as scientific evidence grew some changes in diet were steadily taken up. Flour, beans, bean oil, and pork were recommended instead of rice and salted fish. At this point, the colonial doctors were increasingly confident that the disease could be prevented through a healthy diet, but they also continued to believe there was a link to improvements in sanitation.
In the 1890s, as head of the Dokter Djava School in Jakarta, Eijkman’s research found that a certain substance, which he called the ‘anti-beriberi factor’ was present in unpolished rice but disappeared once it was polished, triggering the disease. This substance was later identified as vitamin B12 or thiamine and his discovery changed modern medicine. Rather than being a disease caused by germs spread from one person to another, vitamin deficiency was responsible for the illness. Despite the many dead ends and mis-directed investigations, perhaps the world also owes a debt of gratitude not just to Eijkman, but also to the unnamed doctors and scientists and their patients in the colonies of Southeast Asia involved in the long search for a cure for beriberi.
Nia Deliana is a lecturer in the Faculty of Social Sciences at the International Islamic University of Indonesia (UIII).